Gordon Brown is facing a damaging rift with his party after slowing the pace of reform in the NHS, The Times has learnt. Private companies and charities are being frozen out of the NHS, prompting accusations that the Government has bowed to pressure from the unions. Andy Burnham, the Health Secretary, is facing a Cabinet backlash, criticism from the former ministers John Hutton and Alan Milburn and attacks from the CBI and charity groups over proposals to limit outside involvement in the NHS.
The Department of Health will publish new guidelines shortly that limit private companies and charities to providing services not already offered or in areas where the existing NHS is failing. A draft obtained by The Times says: “Only if there was insufficient improvement within a reasonable timescale and the scale of under-performance was significant would the PCT [primary care trust] consider engaging with other potential providers or other solutions (eg, franchising).”
This is regarded as a dramatic shift from the policy set out by Alan Johnson when he was Health Secretary. His document, Necessity Not Nicety, suggested that primary care trusts should become more competitive and commercial, but Mr Burnham is understood to think that this unsettled the health service.
Mr Burnham’s change is regarded as a political manoeuvre, with both the Conservatives and the Liberal Democrats pledging to make it easier for outside organisations to provide work for the NHS. Civil servants have said privately that sections in the new guidelines referring to the NHS as the “preferred provider” have been pre-negotiated with unions and should be regarded as untouchable. Some NHS trusts are not waiting for the new guidance, though, and are already abandoning plans to use outside providers.
The move has caused tensions at Cabinet level, prompting a disagreement in one Cabinet sub-committee during which Mr Burnham was accused of going back on new Labour’s modernising agenda. Blairites suggest that attempts to “buy off” Unison and Unite, which together provided £6.6 million to Labour — around 30 per cent of its income — in the year to June, are damaging the party.
Documents uncovered by Norman Lamb, the Liberal Democrat health spokesman, suggest that Mr Burnham has met union representatives more than any other group since he became Health Secretary in June. The Department of Health is refusing to release the notes of one meeting that took place September, claiming that they are subject to “Chatham House” rules that secure anonymity. In a letter to Brendan Barber, TUC General Secretary, Mr Burnham appeared to acknowledge that TUC staff were involved in helping to draw up the policy by thanking them for their work.
“This is a perfect illustration of the corrupting influence of big money in politics,” Mr Lamb told The Times. “This move will undermine the efforts to improve efficiency and productivity in the NHS.”
Representatives of the NHS Confederation, CBI and Acevo, which represents charities, are still battling to water down the guidelines before publication, asking why the outside groups should only be be approached when the NHS has failed.
Stephen Bubb, chief executive of Acevo, said: “This is a clear breach of the Government’s manifesto promise that the third sector will be treated as an ‘equal partner’ in providing services.” Susan Anderson, CBI director of public services, said: “These are more designed to assuage the demands of trade unions than to meet the needs of patients.”
There is also tension within Labour, with concerns expressed by at least two Cabinet ministers and pressure on Lord Mandelson to overturn the shift on the grounds that it might break government competition guidelines and EU competition law.
Mr Hutton told The Times: “I would be concerned about any policy that turned the clock back because you can’t.” Mr Milburn has already attacked the plans, saying: “There should be no preferred provider. Quality should be the only yardstick, not the type of provider.”
Two former government advisers, professors Julian Le Grand and Paul Corrigan, have also criticised the move.
A spokeswoman for Mr Burnham denied that they were bowing to pressure from the unions. “When services are performing well, and we’ve invested a lot of money in them, why would you pull the rug from under the NHS and put services out to tender?”
She strongly denied any accusation that the party was doing the bidding of the unions, and said that the new rules could mean that outside providers received more work from the NHS rather than less. “We are not bound by either the unions or outside groups and we want to have a good relationship with all of them.”
SOURCE
Another cancer drug too dear for Britain: Bowel cancer victims denied life-prolonging care that's free in Europe
Bowel cancer sufferers are to be denied a life-prolonging drug on the NHS which is available to patients across Europe and beyond. Trials show Avastin can extend life by almost two years. But the Government's rationing body, Nice, says it is not cost-effective.
In what has been dubbed 'passport prescribing', Britain does not allow routine use of the drug while patients in virtually all other EU countries get the drug paid for. France, Germany, Italy and Scandinavian nations, as well as Australia and Canada, all meet the cost of treatment.
Around 35,000 Britons develop bowel cancer each year, of which 4,000-5,000 with advanced cancer could benefit from the drug. Avastin, also known as bevacizumab, costs around £18,000 for a course of ten months' treatment given as intravenous infusion with chemotherapy. The price is similar to that in other countries.
But the complex formula used by the National Institute for Health and Clinical Excellence, which looks at quality of life and overall cost effectiveness, says the annual cost is £36,000. This breaks the maximum limit set by Nice of £30,000 - a figure which has not changed in ten years despite inflation.
Although the manufacturer Roche devised a subsidy scheme to reduce an original Nice estimate from £62,000 in an attempt to get it approved, this was not good enough. Nice's decision, which is preliminary, puts Britain in the same category as Latvia, Poland, Albania and Macedonia in not paying for sufferers to use the drug.
Last night patient groups and experts voiced their dismay. Kate Spall, of the Pamela Northcott Fund, which assists cancer patients denied new therapies, said: 'This is another bad day for cancer patients and another good day for accountants.'
Professor Will Steward, of the Department of Cancer Studies and Molecular Medicine at Leicester University, also said he was disappointed. 'Having Avastin would bring new hope to the many patients for whom this offers a proven increased chance of living longer with a better quality of life,' he said.
Dr Rob Glynne Jones, chief medical adviser of the Bowel Cancer UK charity, called for Nice, the manufacturer and the Department of Health to find a compromise that would allow the drug to be used. 'The clinical efficacy of bevacizumab and its benefit to patients with metastatic colorectal cancer is well proven,' he said.
Patients waiting for a decision on Avastin are forced to plead for special funding from local health bodies or hope that a trial of the drug is running in their area.
Nice, which has been accused of spending more on spin than on evaluating drugs, has often been criticised for banning drugs from NHS use as too expensive. Last week it decided to reject NHS use of the liver cancer drug Nexavar, which gives patients six months' extra life. The decision is being appealed.
It contrasts with the fast-tracking of the breast cancer drug Herceptin after pressure from patients and the intervention of the then Health Secretary Patricia Hewitt. Ironically, Avastin also treats breast cancer but its use on the NHS is in limbo until the bowel cancer issue is settled.
Last year Professor Mike Richards, the National Cancer Director, called for greater flexibility between Nice and the pharmaceutical industry to make more treatments available to cancer patients.
Bowel cancer patient Barbara Moss, 54, from Worcester, spoke at a Nice review last month about how Avastin had transformed her quality of life. She was given just five months to live when diagnosed with bowel cancer in November 2006, but is convinced the drug has kept her alive and in remission. She fought to get back from the NHS almost £14,000 sent on ancillary care, but had to pay £9,000 for the drug itself. Yesterday she called on Nice to find a way to approve the use of the drug 'so that thousands can benefit from the drug like I did while avoiding financial hardship'.
Avastin works by blocking the blood supply to the tumour, starving it of oxygen and nutrients. Once it has shrunk it can be surgically removed.
Dr Carole Longson, director of the health technology evaluation centre at Nice, said its decision was preliminary. While it recognised that the drug 'may provide benefits in terms of clinical effectiveness', it concluded that 'the high cost of bevacizumab relative to the benefits it brings means that it is not a cost-effective use of NHS resources'.
SOURCE
British woman saw seven different government doctors but not ONE spotted her brain tumour
Diagnostic tests? Forget it! Sprinkle lavender oil on your pillow, she was told. She was even seen by a specialist but still no scan
When Nicole Witts complained to her GP about excruciating headaches she was told it was sinusitis. When, four months later, she asked why her arms were going into spasm she was told she probably had a trapped nerve. Over the course of five months, Nicole, 37, a mother of two, saw eight different doctors who came up with a range of diagnoses - including post-natal depression - but all of them failed to spot the truth: Nicole had a brain tumour.
By the time it was detected, in February 2008, the tumour was the size of an orange. Even then, doctors picked it up only because Nicole had had a massive fit and was rushed to hospital by ambulance. A brain scan revealed the tumour over her left ear.
'When the doctor told me what they'd found, I thought: "Oh God, I'm going to die",' recalls Nicole. 'I am not normally religious, but over the next few days I spent most of my time, when not in bed, in the hospital chapel. 'I was so frightened - not for me, but for my kids, wondering how they would cope without their mum.' Her daughters Megan and Ellen were then only four and eight months old
'I had suspected for some months there was something wrong with me, but the way the various doctors had repeatedly dismissed me had left me wondering if I was going mad. 'Yet despite the awful news, I was relieved to know that I hadn't been imagining it all.'
With brain tumours, early diagnosis can be a matter of life and death. Around 16,000 people in the UK develop a primary brain tumour each year and around 3,500 people die as a result, often because the tumour is detected too late for it to be treated effectively.
Many of these are not cancerous - which can spread elsewhere; instead, they are benign growths that have formed around vital areas of the brain. But though 'benign', these growths can cause irreparable damage to blood vessels, causing bleeding in the brain, or a build-up of fluid, or exert pressure on vital parts that control nerves and signals.
No one knows what causes primary brain tumours. The symptoms vary according the tumour's location. Although persistent headaches are the most well known - and the symptom that frightens patients most - they occur only in one in three cases. Nausea, balance problems, weakness in the limbs, pins and needles and concentration problems are among other possible symptoms. Tumours can also cause disturbance to vision, and are sometimes detected by opticians.
One of the most common symptoms is a fit, as in Nicole's case. This occurs when the tumour applies pressure to sensitive areas of the brain, interrupting the electrical and chemical messages that pass between the brain cells.
Nicole believes hers would have been diagnosed more quickly if she had consistently seen the same GP during her visits. But she belongs to a large surgery with nine doctors, of whom she saw seven. She also saw a hospital ear, nose and throat specialist. 'Each doctor I saw had a different theory about what was wrong with me. The range of possibilities they came up with was amazing. 'If we still had the old fashioned practice, where you see only your own GP, I think my tumour would have been picked up sooner.'
Nicole's experience is quite common. 'We get a lot of calls about this,' says Moira Dennison from Brain Tumour UK. 'This lack of continuity of care means tumours aren't picked up until later than they should be. 'People see one GP and then another and then another and no one is putting all the information together that points to a brain tumour.'
It's the system that is at fault, says Dr Steve Field, chairman of the Royal College of GPs, not GP training. He explains that it's designed so 'patients can quickly get to see a doctor', but this creates problems with lack of continuity of care. 'If, as a doctor, you see a patient repeatedly you build up a rapport with someone and get to know them. Then, you would most probably pick up a problem earlier than if you saw someone on a one-off basis. 'My advice is that if you have something persistent you should wait to see the doctor you saw before.
He adds: 'Headaches are far more common than brain tumours and, if anything, doctors over-diagnose the possibility of brain tumours and so a lot of people who don't have a brain tumour are referred for investigation.' However, this was not the case for Nicole - indeed, at one point a GP laughed about her symptoms when she tried to make an appointment.
Nicole, from Leighton Buzzard, Beds, first went to see the doctor in August 2007 when she found her hearing had become muffled and she was hearing whirring noises in her head. 'I didn't have a clue what was causing it, but when I saw the doctor I tapped the side of my head where I now know the tumour was growing and said: "It feels as if there is something in there",' Nicole says. 'However, the doctor thought it was sinusitis and gave me a nasal spray. I didn't think it sounded right - I didn't even have a runny nose. 'I used the spray for two weeks with no joy, so another doctor referred me to hospital because my hearing was still muffled.
'I was seen by an ear, nose and throat specialist who thought I had an infection that had caused a build-up of fluid behind the ear - and suggested I have an operation to have a grommet (a small plastic tube) to drain the fluid. 'I had that done and it did partially improve the muffled sensation, though no one is sure why.
'However, by the autumn I began to get headaches which were so severe I could hardly put my ear on the pillow at night. They were crippling. Later, I found out this was because the tumour was putting undue pressure on certain areas. 'However, when I went back to the surgery - and saw yet another GP - he thought it was maybe due to stress and suggested I try sprinkling lavender oil on my pillow to help. 'Looking back, it is laughable, but we are programmed to accept what doctors tell us and so I did.' ....
Nicole needed major surgery to remove the tumour and had to be transferred to the Royal Free Hospital in North London. 'The surgeon told me the tumour was almost certainly benign, but it was huge and would need a nine-hour operation to remove it,' says Nicole. 'I was relieved it wasn't cancerous, but I was still really worried. 'He told me if I didn't have it removed then I would be dead within six months - because although it was benign, it would cut off the blood supply or cause bleeding. The surgery had a one per cent risk of death and a five per cent risk of paralysis, but I knew there was no alternative.'
Nicole had the operation on March 14 last year. 'The surgeon came to see me afterwards and he was really excited because he had managed to get all the tumour out. 'It was a huge relief. Gary was there and I instantly recognised him. He was so relieved, not just that I had come through the operation, but also that I was still "me".' A week later, though still very fragile, Nicole was allowed out of hospital.
'There is a 30 per cent chance that the tumour will return. I will have to have an annual MRI scan for five years, but I prefer to think of it as there being a 70 per cent chance that it is gone for good.'
Meanwhile, Nicole is still living with the consequences of her late diagnosis. Her short-term memory has been affected because the tumour damaged the part of the brain which is responsible.
More here
Rasmussen: Support for Health Care Plan Falls to New Low
Just 38% of voters now favor the health care plan proposed by President Obama and congressional Democrats. That’s the lowest level of support measured for the plan in nearly two dozen tracking polls conducted since June. The latest Rasmussen Reports national telephone survey finds that 56% now oppose the plan.
Half the survey was conducted before the Senate voted late Saturday to begin debate on its version of the legislation. Support for the plan was slightly lower in the half of the survey conducted after the Senate vote. Prior to this, support for the plan had never fallen below 41%. Last week, support for the plan was at 47%. Two weeks ago, the effort was supported by 45% of voters. Intensity remains stronger among those who oppose the push to change the nation’s health care system: 21% Strongly Favor the plan while 43% are Strongly Opposed.
Rasmussen Reports is continuing to track public opinion on the health care plan on a weekly basis. Next week’s Monday morning update will give an indication of whether these numbers reflect a trend of growing opposition or are merely statistical noise.
Only 16% now believe passage of the plan will lead to lower health care costs. Nearly four times as many (60%) believe the plan will increase health care costs. Most (54%) also believe passage of the plan will hurt the quality of care.
As has been the case for months, Democrats favor the plan while Republicans and voters not affiliated with either major party are opposed. The latest numbers show support from 73% of those in the president’s party. The plan is opposed by 83% of Republicans and 70% of unaffiliated voters.
Other recent polling shows that Democrats consider health care reform to be the top priority for the president. Republicans and unaffiliated voters see deficit reduction as most important.
Among the nation’s senior citizens, 34% favor the health care plan and 60% are opposed. A majority of those under 30 favor the plan, but a majority of all other age groups are opposed (Premium Members can see full demographic crosstabs).
Support for health care has declined along with President Obama's approval ratings. For the first time in the Obama era, the Rasmussen Reports daily Presidential Approval Index has been in negative double digits for nine straight days.
Despite the decline in support for the health care plan, 50% still say it is at least somewhat likely to become law this year. That figure includes 17% who say passage is Very Likely.
While Senate Democrats this weekend assembled enough votes to begin debate on the plan, many challenges remain. All Republican Senators and several Democrats, for example, have expressed opposition to the so-called “public option.” Sixty-three percent (63%) of voters nationwide say guaranteeing that no one is forced to change their health insurance coverage is a higher priority than giving consumers the choice of a "public option" government-run health insurance company. Most liberal voters say giving people the choice of a "public option" is more important. But most moderates take the opposite view and say guaranteeing that no one is forced to change their health insurance is the top priority.
Overall, 46% favor the creation of a government-sponsored non-profit health insurance option that people could choose instead of a private health insurance plan. However, if the plan encouraged companies to drop private health insurance coverage for their workers, support for the public option falls to 29%, and opposition rises to 58%.
As Scott Rasmussen, president of Rasmussen Reports, wrote in the Wall Street Journal: “The most important fundamental is that 68% of American voters have health insurance coverage they rate good or excellent. … Most of these voters approach the health care reform debate fearing that they have more to lose than to gain.”
Other challenging issues in the Senate debate include abortion and illegal immigration. Ever since the House's passage of the Stupak Amendment which says the "public option" would not cover elective abortions and that recipients of federal insurance subsidies could not use them to buy abortion coverage, the divide among Democrats has been visible.
Earlier polling showed that 48% nationwide favored the abortion ban, but most supporters of health care reform didn’t want to address the issue. Just 13% of all voters wanted abortion coverage mandated in the legislation.
On immigration, 83% say that proof of citizenship should be required before anyone can get health care assistance from a government program. Most Democrats while claiming the plan will not cover illegal immigrants are opposed to including a proof-of-citizenship stipulation.
Other polling shows that 47% trust the private sector more than government to keep health care costs down and the quality of care up. Two-thirds (66%) say an increase in free market competition will do more than government regulation to reduce health care costs.
While voters are skeptical of the plan working its way through Congress, 54% say major changes are needed in the health care system. Sixty-one percent (61%) say it’s important for Congress to pass some reform. Only 31% believe Congress has a good understanding of the proposed health care reform.
SOURCE
Surgeons angered by proposal for tax on plastic surgery
A tax on being unattractive? Where is the Democrat "compassion" in that?
Plastic surgeons are angry over proposals for a 5 per cent tax on their business. Although encouraged by politicians to put a brave face on it, plastic surgeons across America are outraged by proposals for a 5 per cent tax on their business. Senators hope that the tax, which was buried in a 2,000-page healthcare Bill released last week, will help to pay the $850 billion (£510 billion) cost of overhauling the country’s medical system.
However, doctors and medical product companies attacked it as discriminatory against women, who make up 86 per cent of cosmetic surgery patients, and likely to fail in its aims. They said that state tax auditors, not doctors, could end up deciding whether operations were necessary for cosmetic or medical purposes.
The Senate Bill contained scant detail on the proposed tax, other than that it would apply to procedures that were not treating deformities created by congenital abnormalities, injuries or disfiguring diseases. Nicknamed Bo-tax, it could raise $5.8 billion over ten years for the Government and would come into effect in January, paid by patients and collected by doctors.
Amit Hazan, an analyst at Oppenheimer, a financial adviser, said that the tax would collect about $60 million a year on Botox treatments alone, while breast implant surgeries would raise $110 million. Customers of Allergan, the maker of Botox, could be hit with about $120 million of tax in a single year, he said. A spokesman for Allergan described the tax as a “random hit on an easy target that is only punitive and not corrective. It has nothing to do with reducing healthcare costs or trying to change unhealthy behaviour.”
Jonah Shacknai, chief executive of Medicis, accused Democrat senators of making moral judgments about people who had cosmetic procedures.
Harry Reid, the Senate Majority Leader who introduced the Bill, appeared unrepentant. When asked to justifty the tax, a spokeman for his office said: “We needed money.”
SOURCE
Have Democratic Leaders Gone Mad?
With the introduction of Harry Reid's health care bill - talk will inevitably focus on whether the public option or the Stupak amendment will undermine the legislation. Yet, if the bill dies, I do not think either of these will be the primary cause of death. I think this will be the culprit:
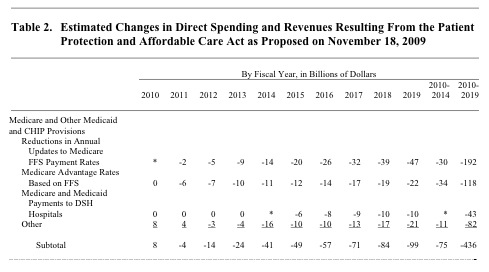
This is the CBO's analysis of how the Reid bill will cut Medicare. The total reductions come out to $491 billion over 10 years when everything is factored in. The following has been said by other commentators, but I have to add my voice to the chorus: This is insanity, Democratic leaders. Why are you doing this?
Getting AARP's support might give you cover among the Washington crowd, but let's inject some common sense here. Lots of people are members of AARP, but that does not mean they are intensely committed to it, and will therefore follow its lead on such an important issue. AARP is not like the unions in that regard. Lots of people join to get discounts on auto insurance and movie tickets, meaning that affiliation with the organization is broader than it is deep.
Obama's current numbers among senior citizens demonstrate the validity of this point, not to mention the concern that Democrats should have heading into 2010. Gallup has him at 45% among those over 65, and at 49% among those between 50 and 64. Hint. Quinnipiac has him at 42% with those over 55. Hint hint. Rasmussen currently shows Democrats losing the generic ballot among seniors by 15 points; in 2008, Democrats split the senior vote with the GOP. Hint hint hint.
Let's review the political power that American seniors wield. In the Virginia gubernatorial election, people over 65 accounted for 18% of all voters. In New Jersey it was 19%. People over 65 accounted for 19% of all voters in the 2006 House midterm. And even in the "Yes We Can!" presidential election of 2008, when college kids supposedly overwhelmed the normal electoral process, the 65 and over crowd still accounted for 16% of the electorate (unchanged relative to 2004).
The 2006 House exit poll showed the Democrats winning the national vote by a margin of 54 to 46. If, however, we plug in Rasmussen's current generic ballot number among seniors in place of what the Democrats actually won from that cohort in 2006, their lead falls to 52-48. Note that this assumes no change among younger cohorts. That's seniors alone cutting the Democratic margin in half. This also assumes that seniors do not come out in greater numbers in 2010 to defend against perceived assaults on their Medicare benefits.
Blanche Lincoln knows what I'm talking about. When she won reelection in 2004, seniors made up 16% of the electorate and went 59-41 for her. In the 1998 midterm, seniors made up 26% of the electorate and went 60-37 for her. In both contests, they were her strongest supporters. I wonder what she thinks of Table 2 in the CBO's analysis of the Patient Protection and Affordable Care Act.
Bob Dole knows what I'm talking about, too. From January through September of 1995, Bill Clinton's job approval numbers were tepid, with a typical net approval rating of about +2.5. Things turned around for him in late 1995 when the budget battle heated up and Clinton took a stand against...GOP reductions in projected Medicare spending! I'll let Michael Barone finish the story. This is from the 1998 Almanac of American Politics:
[I]n August 1995 [Clinton] started running political ads against the Republicans' Medicare plan. All this was part of a strategy pollster Dick Morris called "triangulation," taking positions between liberal Democrats and conservative Republicans so as to elevate the president's stature above both...In November and December he negotiated on the budget with Speaker Gingrich and Senate Majority Leader Bob Dole, promising them agreement at times, but he ultimately vetoed most of their appropriations bills. That technically shut down non-emergency functions of the federal government, a step which many Republicans initially welcomed and thought would be popular. This was a stunning miscalculation, as was their lack of a strategy to deal with Clinton's vetoes...By the time Republicans backtracked and agreed to Clinton's terms, their ratings were down and they were running behind Democrats in the polls.
The President declared at the time the deal was struck that his proposal was a "sensible solution" that showed "you can balance the budget in 7 years, and protect Medicare and Medicaid, education and the environment and provide tax relief to working families." He cruised to reelection.
Not coincidentally, Dick Morris was the first to suggest that mucking around with Medicare would mean trouble for the Democrats. He knows what he's talking about, and in September he wrote:
"The Democratic Party, led by Obama, is systematically converting the elderly vote into a Republican bastion. The work of FDR in passing Social Security in 1937 and of LBJ in enacting Medicare in 1965 is being undone by the president's healthcare program. The elderly see [Obama's] proposals for what they are: a massive redistribution of healthcare away from the elderly and toward a population that is younger, healthier and richer but happens, at the moment, to lack insurance. (Remember that the uninsured are, by definition, not elderly, not young and not in poverty - and if they are, they are currently eligible for Medicare, Medicaid or SCHIP and do not need the Obama program.) The elderly see the $500 billion projected cut in Medicare through the same lens as they viewed Gingrich's efforts to slice the growth in the program in the mid-1990s.
Why are Obama, Pelosi, and Reid doing this? How could they be so foolish as to repeat the most egregious mistake of the Republicans of the 104th Congress? Why are they forcing their vulnerable members to vote on a bill that would cut Medicare in this fashion? Do they dislike their moderate colleagues? Do they find the chore of being the majority party too burdensome? Have they simply gone mad?"
SOURCE

No comments:
Post a Comment